

If you want to search Cost Curve back issues or link to anything you read here, the web links and archive are online at costcurve.beehiiv.
We’re not done with smoothing -- ahem, M3P -- quite yet.
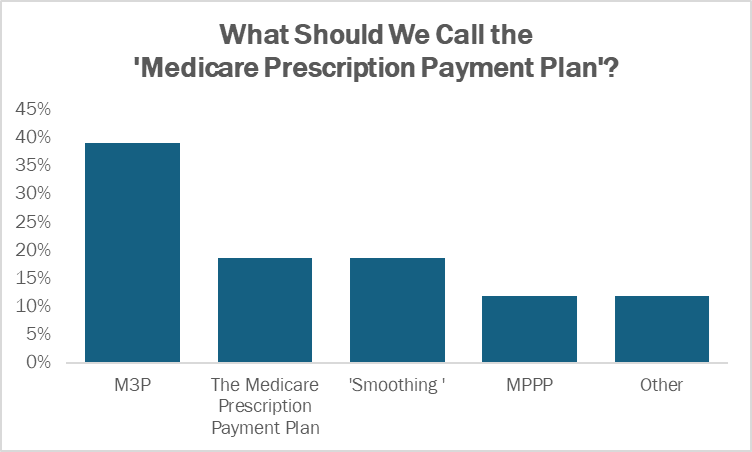
First off, I have results from yesterday’s poll: you are all overwhelming in favor of “M3P” as the best way to reference the Medicare Prescription Payment Plan, with nearly half of the votes supporting that particular abbreviation.
There were some comments that suggest that maybe MP3 would be even better. That one has a kind of Napster throwback feel, but I fear that the market has spoken.
Because you are all thoughtful readers with an eye toward communications, many folks flagged that the program’s full name needs to be included when speaking with consumer audiences about the M3P, and that a fuller, wordier description of what the Medicare Prescription Payment Plan actually is is probably warranted, too.
After all, the readership of Cost Curve is probably not hugely representative, and as much as sling around abbreviations will make us feel cool and wonky, it’s not going to help patients understand.
Second, there have been some other attempts to educate on exactly what M3P is and how it will work, with this Alliance for Patient Access fact sheet as the latest entrant. There is a temptation to pass judgment on all of these patient-focused materials because it’s impossible not to err on either the side of over-simplification or borderline-confusing.
My take is that as long as you’re not leading consumers astray -- e.g. the CMS “Will this payment option help me?” tool -- the more information that is out there, the better.
Print this out for your weekend reading list: it’s a paper from Lou Garrison and some other folks, including a BMS exec, that describes the underlying economics of drug development. It’s a good reminder that a) there’s only a fairly narrow window for medicines to generate profits for their inventors, and b) most medicines don’t make back their development costs. These are not profoundly novel concepts, but they often go out the window when discussing drug prices, so a good, clear refresher should be welcomed.
Important Mercer report here on health insurance costs for employers, showing that costs will be up 5.8% next year, the third straight year of 5%+ increases. (The trend, in the decade prior, was around 3% a year.) The area of largest growth is in prescription drugs. I suspect that employers are going to get increasingly loud about this trend, which has the possibility of overflowing into everything from PBM operations to a closer look at 340B.
Speaking of overflowing: one way of trying to address increases in spending on pharmaceuticals is to go after doctors who prescribe GLP-1 medicines. That’s what Anthem is doing, per a wild Bloomberg story that says that the insurer is accusing doctors of falsifying records to get reimbursement for the meds. The docs deny the allegation, and a benefits consultant called the move “weird.” (“Weird” being the putdown of the year for 2024.)
There seems to be something of an early-stage research slowdown -- due in part, probably, to IRA-related factors -- though the evidence remains circumstantial. Still, that pile of circumstantial evidence is growing, with the announcement of layoffs at Charles River Labs one more piece of the puzzle.
Sen. Peter Welch introduced a Senate version of the 340B Patients Act, which is the massively pro-hospital 340B bill already circulating in the House. I’m hesitant to call it a “reform” bill because it dodges all of the big questions swirling around the program, but it gives the hardcore hospital partisans something to advocate for. My assumption is that this is a DOA bill, legislatively, that will nonetheless be used as a messaging weapon for one side of the conversation.
Thanks for reading this far. I’m always flattered when folks share all or part of Cost Curve. All I ask is for a mention or tag. Bonus points if you can direct someone to the subscription page.
