

If you want to search Cost Curve back issues or link to anything you read here, the web links and archive are online at costcurve.beehiiv.com. You can subscribe there, too.

Four times a year, I holler and moan about UnitedHealth Group’s quarterly earnings, which are always, always good, even a few months after a system-crippling hack. This quarter: $4.2 billion in profits.
I always worry about coming off as hypocritically anticapitalist, and I don’t want to suggest that health insurance cannot or should not be a for-profit enterprise. It’s just that -- damn -- there is a lot of money sloshing around at a time when it feels like health insurance services are getting worse.
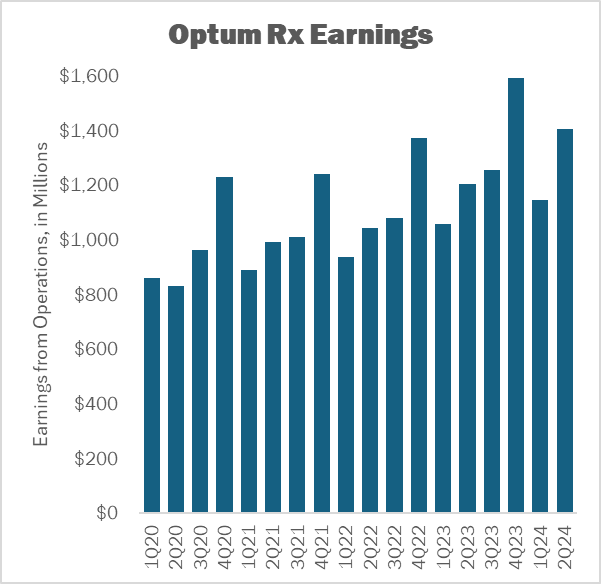
I also went and looked at earnings from operations for United’s PBM, Optum Rx. Again, we’re in a period in which PBMs are under incredible scrutiny, and if ever there was a time to invest revenue in making the PBM work better for patients and employers, now would probably be the time.
Instead, United booked record revenue for Optum Rx -- $32 billion -- of which $1.4 billion ended up as earnings.
What did the health system get for that $1.4 billion? Hard to say. But investors loved it. The market cap of United, as the moment I’m writing this, is up more than $20 billion on the day.
I’m really taken by the 340B/IRA math in this great LinkedIn post by attorney Bill Sarraille.
I can’t do the underlying calculus justice -- it’s worth surfing over and checking it out yourself -- but the quick upshot is that covered entities buy about $10 billion worth of the 10 medicines getting price controlled. They make about $6 billion a year on the usual 340B arbitrage.
By Sarraille’s estimates, 340B hospitals will only end up with about $2.5 billion in revenue from those 10 drugs after the IRA’s “maximum fair prices” kick in. That leaves a $3.5 billion hole.
With me so far? Because this is where it gets interesting.
340B advocates have warned that the IRA “negotiations” will prompt a shortfall of $1 billion (or so). Sarraille is estimating a much bigger gap. What gives?
Well, covered entities won’t take the same hit if patients are on more expensive, non-price-controlled drugs. Sarraille posits that if 340B providers can move 75% of patients off of the 10 “selected” drugs onto similar (but more costly) therapies, they can blunt that impact … and get the total “cost” closer to $1 billion.
These are all back-of-the-envelope calculations, but even if Sarraille’s numbers are off a bit, it still suggests that hospitals are going to try to move huge numbers of patients onto more expensive drugs, because that’s what the 340B program incentives.
This is -- ironically -- the system at work.
I’d like to write something more piercing about where newly minted Republican VP nominee J.D. Vance stands on various drug-pricing issues, but it turns out there’s not much to go on. On the one hand, the dude is a biotech investor, so he presumably knows how the industry works. On the other hand, he gave an interview to the AARP where he articulated something that sounds like a lot like Joe Biden’s worldview:
“I think we have to let Medicare negotiate prescription drug prices so that our seniors aren’t paying through the roof for prescription drugs. … In addition to allowing Medicare to negotiate prescription drug prices, we need to allow American companies and pharmacies to import drugs from overseas. Europe pays way less for drugs, even drugs that were developed in the United States, than America pays. So a lot of Americans, especially American seniors, are subsidizing European health care. We have to have leaders who look out for our citizens first, and one of the ways is allowing drugs that are being sold at a certain price in Europe to come into our country to be sold at the same price.”
Maybe that was just campaign-season pandering to the AARP, but Vance has refined a certain brand of populism that suggests that he may not be a great defender of innovation.
Elsewhere:
J&J and BMS filed the first briefs in the appeal in their case challenging the IRA. Bloomberg Law has coverage. The arguments look pretty similar to those deployed at the district court level, so my guess is that there won’t be any real drama here until we hear from the judges.
Usually, when health policy topics are discussed in the Journal of the American Medical Association, it’s old news. But understanding the perspectives that doctors are exposed to is not unimportant, so it’s worth flagging that JAMA just published a “Viewpoint” that takes a sympathetic tone to using march-in rights as a price-control tool.
Yesterday, I wrote about the “profoundly dystopian” reality of “deductible parties” in the United States. It must be a week for dystopia, because -- in the UK this time -- there is a patient-advocacy effort by breast cancer advocates to gain access to the breast cancer drug Enhertu, which has had blowout data but won’t be reimbursed by the NHS. So the advocates have taken to going topless to make their point. It’s done a great job of garnering press, but it’s probably a sign that we’re not having the data-driven discussion that’s really needed.
I’m not sure what to make of new Gallup numbers that show that Americans kind of trust the health care system, especially given that other Gallup polls show that Americans have a pretty dim view of the industries that constitute health care. Jane Sarasohn-Kahn has a good perspective on that disparity and why there are seeds for optimism in all these numbers.
Header image by Giorgio Trovato on Unsplash.
Thanks for reading this far. I’m always flattered when folks share all or part of Cost Curve. All I ask is for a mention or tag. Bonus points if you can direct someone to the subscription page.
