

If you want to search Cost Curve back issues or link to anything you read here, the web links and archive are online at costcurve.beehiiv.com. You can subscribe there, too.

I’m still stuck on 340B.
***
340B Report has the reaction of the covered entities to the HRSA numbers. And the response here is illuminating.
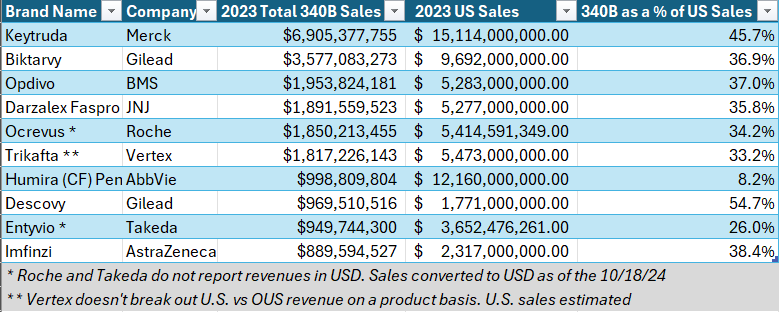
Hospital reps are telling the outlet that the stunning year-over-year increase is due to increasing prices. This is not remotely true. Take Keytruda, the #1 340B drug. It saw two price hikes of 2% last year. That doesn’t get you to a 24% increase. Ditto Biktarvy, the #2 drug, which was at a 5.9% increase for the year. (That’s at list price. I assume any net price increase was much thinner.)
There was also some hand-waving from the 340B community about inpatient versus outpatient spending, but that’s not a trend that’s specific to 340B, and we’re not seeing Medicaid budgets or Medicare spend (for example) getting blown up in the same way.
The reality is that, yes, use of targeted oncology meds is growing quickly everywhere. But that doesn’t take away from the fundamental fact that 340B revenues are growing. And it doesn’t make the question of where those dollars are going go away.
Talk about phony “exploding” drug prices is a pretty good tell: 340B hospitals have zero interest in talking through what’s actually going down.
***
Jake Auchincloss, a member of Congress from Massachusetts, posted a poll on LinkedIn yesterday asking for perspective on what was going to finally solve the 340B issue. You should go vote in that poll. (You should go vote for president, too, but that’s another conversation.)
The objectively right answer to Auchincloss’ poll is that Congress is the vector by which all of this gets solved. But I don’t have a lot of faith that Congress is sufficiently motivated to do hard, wonky work that is going to involve kneecapping the politically powerful hospital lobby.
My take is that greater public understanding -- which is code for “media attention” -- is a precondition for congressional action. This is not a short-term proposition. The HRSA number has received exactly one piece of meaningful coverage (props to Ed Silverman at STAT), despite being dramatic and somewhat easy to put in context.
But I’m old enough to remember 2016, when the idea that mysterious entities called PBMs were at the root of the EpiPen pricing controversy was too radical for people to grasp. Now, eight years later, there’s broad understanding of the role of PBMs.
I hope that it doesn’t take a decade for people to grasp 340B, but that’s probably how we need to think about things. The second best time to plant a tree is today.
***
I’m so deep in 340B that I’m seeing echoes in things that are not remotely 340B-ish.
Take KFF’s annual survey of state Medicaid directors which is, as tradition, fairly grim. Despite falling enrollment, about half of all states are worried about budgets next year, and Medicaid directors don’t have that many levers to pull to change the landscape.
One way of taking pressure off of state Medicaid programs would be to look at 340B reforms, because 340B raises prices across the system in a way that boomerangs back to hurt Medicaid. This phenomenon is laid out well in this analysis by Health Capital Group.
I don’t think that’s the silver bullet that will turn the tide around 340B, but I suspect that a growing awareness the 340B abuse is not a victimless crime only pushes us closer to a turning point.
FDA chief Rob Califf doesn’t like the price of obesity drugs, per Endpoints. While I don’t doubt the sincerity of Califf’s feelings here, there’s a certain irony. Cost-effectiveness is a function of (duh) cost and effectiveness, raising an interesting question: is the FDA doing everything in its power to make sure that the “effectiveness” part of the equation is fully addressed?
STAT’s take on possible health items that could emerge during the lame duck includes a mention of PBM reform. That’s not a surprise, but I’ll be curious to see how/when this really starts being a part of the talk track of any of the actual decision-makers.
Lots of stats in this Managed Healthcare Executive piece on accumulators/maximizers/alternative funding programs from the AMCP Nexus meeting. The takeaway seems to be that employers plan on continuing to use those tools because of a perception that they deliver savings.
Correction: An astute reader noticed that I had the wrong figure for 2023 U.S. Humira sales in my newsletter on Monday. Below is the corrected chart.
Thanks for reading this far. I’m always flattered when folks share all or part of Cost Curve. All I ask is for a mention or tag. Bonus points if you can direct someone to the subscription page.
