

There is a ton of research in the journals that has hit over the past week or so. It all deserves some visibility and some thought. I’m a big fan of taking time with peer-reviewed research because it ends up being the foundation for future conversations and arguments.
All that to say: this is a necessarily longer Curve today.
If there weren’t such a deluge of research today, I would linger even longer on this JAMA Health Forum paper on one of my favorite topics: launch prices.
The authors look at a relatively simple** set of questions: what did year-by-year launch prices look like in the United States, Germany, and Switzerland, how did those prices change over time, and was there a difference between cancer drugs and noncancer drugs? (In all cases, we’re talking about net prices here.)
The straight-up launch price comparison is interesting, if only because the United States doesn’t show up as much of an outlier as it often does. It also highlights some of the year-over-year variability. In some ways, it’s hard to parse the country-by-country comparisons because the same drugs weren’t approved at the same time in all three geographies.
Anyway, it looks like this:
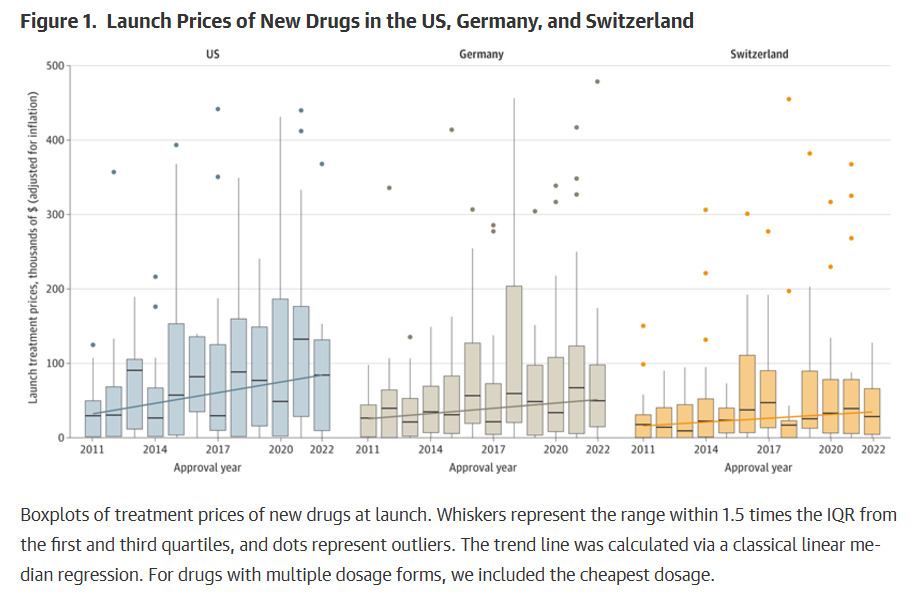
The price-change-over-time is also illustrative: the line goes down in Germany and Switzerland as price negotiations kick in. The U.S. line rises slightly. Again: not a surprise, but well-visualized.
If there’s a takeaway, though, it’s the difference between cancer drugs and noncancer therapies. Naturally, cancer drugs tend to be more expensive -- that’s true in all three countries -- but, over time, in the United States, cancer drugs saw consistent net prices increase, while noncancer meds were flat or falling. In Germany and Switzerland, both groups fell at about the same rate.
Because of the way that the data was analyzed, it’s tough to look at trends over time (the study looks at meds approved between 2011 and 2022). So I’m curious if cancer-drug price hikes have moderated lately. Still, the paper makes a strong case that there is a different drug-pricing dynamic for cancer drugs versus other meds.
** “Relatively simple” is indeed relative: sourcing precise data, especially in the United States, is always tricky. In this case, the researchers used SSR data, which is pretty good, but I’m not sure that I’ve seen it used for launch prices and I don’t have a good sense of what the caveats ought to be there.
***
This is a deeply weird piece, written by a couple of Kaiser Permanente execs and published in Health Affairs Forefront, arguing that the reason drug prices are so high is … the Bayh-Dole Act(?).
Bayh-Dole made it a lot easier for academics to launch their own biotechs, which created a whole drug-development ecosystem that can be directly linked to nearly a half-century of innovation. But the Kaiser guys saw it as the start of an era of bidding wars for innovation that led inevitably to rising prices.
I don’t think that I’ve ever seen Bayh-Dole painted as an original sin, but here we are. (The piece also blames the Medicaid Drug Rebate Program for high prices. Also a weird whipping boy.)
But the real knife twist comes toward the end of the piece, where the execs go after value as a foundation of prices: “This is just industry’s latest attempt to justify prices that are really based on what they think they can get away with.”
Look, drug prices are a legitimate topic of debate. But dismissing value and suggesting that Bayh-Dole is ultimately responsible is kind of a stretch, no?
***
There’s not much commentary to add here, but this brief JAMA article on the first 10 “maximum fair prices” under the IRA is a worthwhile resource. It compares the MFP to the existing estimated net price, the “ceiling price” under the IRA, and the prices in certain international markets. Nothing here is likely surprising or even really new, but this is how a lot of JAMA readers will be exposed to the topic.
A clip-and-save candidate.
***
One of the arguments for why prices are higher in the United States is that we get better access to the good stuff. Approvals for breakthroughs tend to come earlier here. This paper from JMCP tried to check that argument, finding that, eh, Canada has pretty much the same level of innovation available.
Methodological reservations abound and probably undermine the power of the conclusion: the piece considers a drug to be functionally available in Canada if another med from the same class is approved, if a therapeutically similar drug is on the market, or if the med isn’t seen as providing a big benefit. All of those carve-outs are massively in the eye of the beholder and ignore the realities of patient heterogeneity. Sometimes, more really is more.
***
I’m a fan of papers that put cost-effectiveness in context. This is a nifty effort in Value in Health that looks at the health benefits and costs of orphan drugs versus ultra-orphan drugs. Turns out that ultra-orphan meds are generally super-effective but have worse cost-effectiveness than plain-vanilla orphan drugs because of the higher prices needed to incentivize development for small populations.
This is a useful look at the smaller-than-you-think proportion of health spending that goes toward brand-name meds by Peter Kolchinsky. Kolchinsky pegs that number at 8%, and he shows his math.
It’s a lower number than is usually put forth, in part because Peter (correctly) excludes generic drug spend and partly because of the way he mashes together different data sources. But -- regardless -- it’s still a small number. For a deeper spin through the literature here, this NPC analysis is instructive.
ELSEWHERE:
Reuters is kind of breathless about pharma execs pushing the Trump administration for IRA fixes, but nothing in the piece seems particularly surprising or solid. I suppose it’s a sign that industry believes that the political winds might be blowing in their favor, IRA-wise.
My sense is that more employers are figuring out the obesity-med thing, which goes against the narrative in this weirdly headlined USA Today story about insurers pulling back coverage.
The 340B Report reaction story to last week’s 340B transparency report out of Minnesota is worth the click if you’re a subscriber. As it does so well, 340B Report captures what covered entities think. There is some knee-jerk defensiveness about the report as a whole, which doesn’t land as credible. (The effort was well done, considering some of the limitations.) There’s also an extended discussion of how the Medicaid data presented in the report doesn’t suggest evidence of duplicative discounts because of the way that the Minnesota system is structured.
Cost Curve is produced by Reid Strategic, a consultancy that helps companies and organizations in life sciences communicate more clearly and more loudly about issues of value, access, and pricing. We offer a range of services, from strategic planning to tactical execution, designed to shatter the complexity that hampers constructive conversations.
To learn more about how Reid Strategic can help you, email Brian Reid at [email protected].
