
Happy Canada Day to those who celebrate. We stand on guard for thee.

I would love to be able to say something deep and prescient about the Supreme Court’s decision to toss out so-called Chevron deference. For the past 40 years, SCOTUS has given administrative agencies the benefit of the doubt when they interpret laws, but the high court blew up that idea last week.
It’s one of those decisions that’s seismic … but the impact won’t be immediate. Laws aren’t different today. We didn’t all wake up stripped of some fundamental right. But it does create an opportunity to litigate a huge range of administrative actions. We’re just not sure which ones quite yet.
Still, this is an especially big issue in places where systems are propped up by a lot of agency rulemaking. Like, um, health care, where FDA, HHS, CMS, etc. do tons of work filling in holes when implementing underlying legislation.
No one is yet sketching out which exact policies might be on the firing line or how exactly the litigation would go down, but there seems to be a broad consensus that the FDA will be a post-Chevron battlefield. I’ve seen the IRA referenced in several sources as a place where the loss of Chevron might come into play. And elements of 340B might be on shakier ground.
But all of that is somewhat speculative until lawsuits actually get filed. Stay tuned.
It’s expensive to develop new drugs, as every biopharmaceutical company knows. That fact is fairly evident to investors, too, who understand where breakthroughs come from, how much it costs to generate them, and what the return is.
Pinning down how expensive that endeavor is has been a popular pastime, but I’m partial to the thinking of journalist Matt Herper, now at STAT, who has long been a proponent of a very simple metric: look at total R&D spending reported to the SEC and divide by the number of medicines that make over the FDA finish line.
It’s a crude metric that swishes lots of different elements of research together, but it also has the advantage of being comprehensive and hard to refute. About a decade ago, using that metric, Herper estimated that it costs a big pharma company about $4 billion per drug approval.
That’s not an iron law -- a company with a few successful meds will appear a little better; if you look at smaller companies with one, successful program, the cost-per-drug will be much lower -- but it’s a fairly good proxy for what’s going on. On average, we’re talking billions, plural.
And yet there is a concerted effort to try to undermine that basic arithmetic and “prove” that drugs cost less to develop. The latest effort is from government researchers, who did a lot of math -- calculating the expense of clinical trials, folding in the impact of failure, thinking about the cost of capital -- and estimated that a new, approved drug requires about $900 million in investment to get across the finish line.
That’s a number that is plainly wrong, given the R&D spend of the industry and the number of actual approvals. I mean, every drugmaker on the face of the earth would love for it to be right -- if making new drugs were that cheap, we’d be awash in cures -- but it simply doesn’t reflect reality.
There’s a long history of such attempts to unspool the cost of developing medicines, most of which suffer from some of the same inability to fully reflect that reality. (Herper called one such effort “insanely bad” back in the day.)
The bigger question is why showing drug development costs to be low is such an obsession for so many researchers.
I suppose part of the answer is a basic sense of disbelief that drug development is truly that hard or that expensive, especially for those who aren’t sitting at lab benches or designing 20,000-patient clinical trials.
But the larger motivation, I suspect, is that proving that drug development costs are low can be a cudgel to advocate for lower drug prices. After all, if you can make a medicine for less than a billion, maybe cutting the revenue of drugmakers via regulation won’t lead to terrible impacts on the flow of new drugs.
But even if you were to accept the underlying math and conclude drugs really are as easy to develop as the ivory-tower-types believe, it’s still kind of a hollow conclusion because drugs aren’t priced on how expensive they are to develop, but rather other factors (the value they deliver, the size of the patient population, the competition in a class, and so forth).
I’ll leave the last word to Herper, who wrote the line below in 2017, which still holds up today:
“But believing drug prices are too high does not justify coming up with a flimsy figure to counter the drug industry’s arguments about its R&D expense. In fact, recognizing that R&D is extremely expensive is a fundamental fact that explains why drug companies behave as they do.
Drug prices came up in Thursday night’s debate -- Biden dropped two references to the Inflation Reduction Act into his answers, Trump mentioned insulin once -- but let’s be honest: no one paid any attention to that topic in their post-debate hot takes.
Endpoints rehashed the possibility that UnitedHealth Group/Optum will get into the pseudo-drug-company game, flagging the company’s trademark filing for Nuvaila, a would-be company dedicated to “procuring biosimilar pharmaceuticals and selling pharmaceuticals to wholesale pharmaceutical distributors.” But the piece has some interesting comments and perspectives, including from Hopkins’ Ge Bai, who raised the possibility that biosimilars companies may have to go around insurers/PBMs to succeed.
This JAMA Health Forum paper said that prescription drug affordability improved through the COVID-19 pandemic, though the piece doesn’t seem to give any particular reasons why that might have happened.
As suggested on Thursday, the House Ways and Means Committee did indeed pass -- by a healthy margin -- a weak-sauce bill that would allow Medicare to cover obesity meds … but only for patients who enter Medicare already using the therapies.
Endpoints has a piece about Coherus bowing out of the Humira biosimilars business, selling its product off for $40 million. The market probably needs to be winnowed somewhat, but it hardly incentivizes biosimilar development when this kind of thing happens.
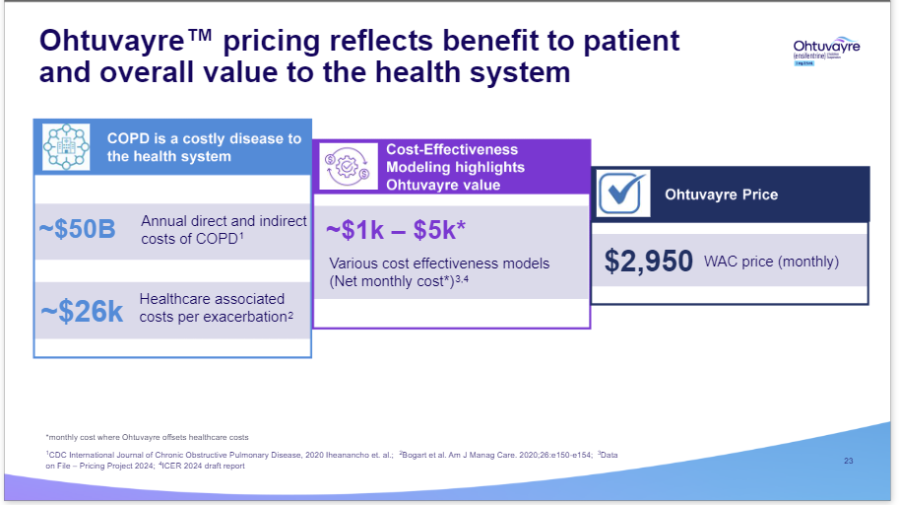
New Drug Price Alert: Verona Pharma won FDA approval for its COPD treatment, which was priced at $2,950 a month. Kudos to the company for being fairly explicit about the drug’s value prop in its approval deck:
Header image via Flickr user Josh Smith.
Thanks for reading this far. I’m always flattered when folks share all or part of Cost Curve. All I ask is for a mention or tag. Bonus points if you can direct someone to the subscription page.
