


The House yesterday passed a mammoth health bill -- including some of the most sweeping PBM regulations ever -- by a huge margin. It includes a ban on spread pricing in Medicaid and some transparency provisions that will give employers a better sense of what PBMs are up to.
I feel like I should be more excited about this, but there are a couple of reasons to keep enthusiasm in check.
First, it sounds (from STAT’s reporting) that there is really no appetite in the Senate to adopt anything the House has put forward. I suppose that’s the nature of sausage-making nowadays.
Second, I’m not certain that these reforms get to the heart of the problem. I don’t think that spread pricing is the kind of widespread issue that it once was. And it’s not clear to me that employers are using the tools they have now to keep PBMs in check, so adding in additional transparency tools feels like a fig leaf.
I give the PBMs credit: they have been able to change their business model quickly and with great savvy, which suggests that nibbling around the edges isn’t likely to make any difference. (And, indeed, if you want to be cynical about it, half-measures probably just give PBMs an opportunity to find more nuanced ways to shift the model to be even harder to force accountability.)
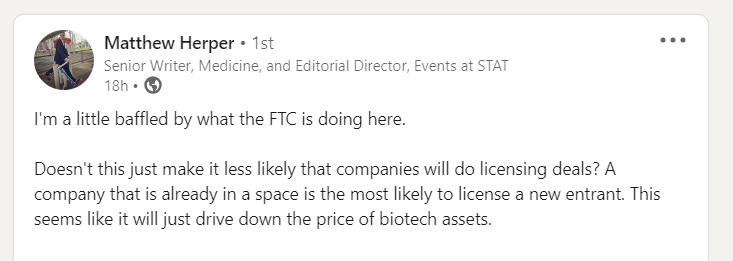
The FTC decided to make it hard for Sanofi to partner with Maze on a new generation of Pompe treatments, so the two companies just dropped the deal altogether.
It’s easy to take aim at the FTC for trying to attack every merger, everywhere, all the time, but this move feels especially pernicious. Companies tend to focus on specific therapeutic areas, not for anticompetitive reasons, but because they can leverage scientific expertise to maximize the value of new discoveries.
I’ll spare you all an extended rant -- though I suspect I’ll have opportunities -- and instead give the floor to someone much smarter than I, STAT’s Matt Herper:
This is an interesting paper on what kind of cancer medicines get the highest prices. It found that small molecules fetch higher prices than biologics, and it concludes that there is no premium for first-in-class drugs. That’s statistically correct -- the difference between first-in-class and next-in-class is not technically significant -- but looking at the charts in the piece, the layperson would certainly conclude that novel meds get higher process. I feel duty-bound to note that the senior author on the paper was Vinay Prasad (IYKYK), so make of that what you will.
AHIP has a new leader: UnitedHealth’s Mike Tuffin. I’m not down with the cast of characters enough to draw any conclusions to that move, but I’m here for any theories or gossip you may have.
There’s an op-ed by an HIV/AIDS activist in Real Clear this morning, castigating hospitals and calling for congressional action. It suffers the same problem that afflicts almost all commentary on 340B: there’s no real solution proposed beyond vague pleas for policy intervention. I’ll probably blow this out in my EOY predictions post, but I think that 2024 is going to be a major year in terms of defining exactly what 340B reform will look like,
I don’t think anything in this CNN overview of the CVS move to “cost-plus” is new, but it gives a nice sense of the shell game that’s being played here: it doesn’t seem like consumers will benefit, and it doesn’t seem like there are overall cost savings, and I’m pretty sure it doesn’t make the system any simpler for anyone. If you wonder why the average American is cynical about the health care system, give ‘em this article and ask for their reaction.
