

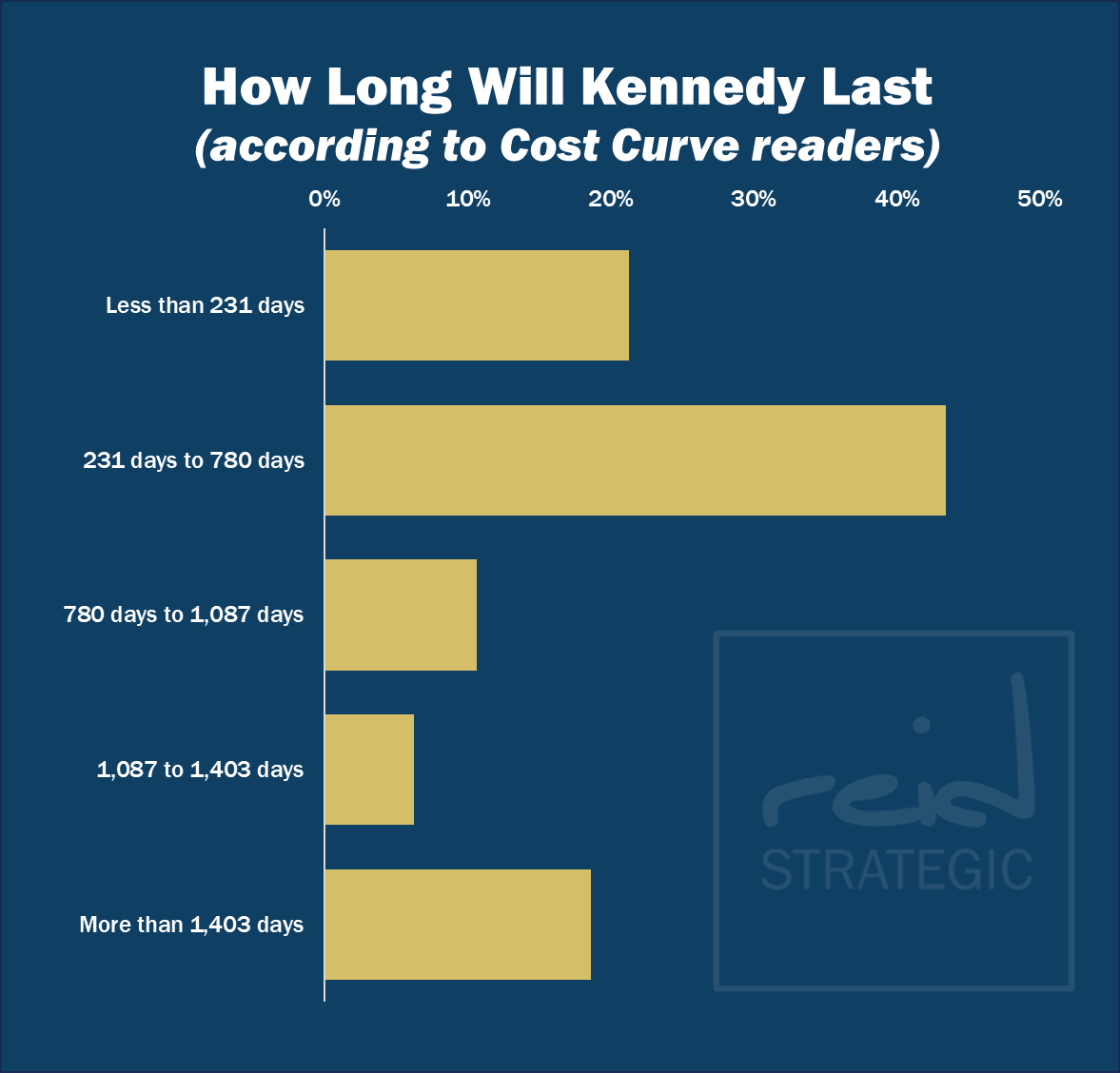
Thanks to everyone who voted in Friday’s poll. Interestingly, those of you who left comments suggested that there wouldn’t be a lot of forces acting to push Kennedy out. And I’m with you. It seems unlikely that a Tom Price-sized scandal would sink Kennedy.
And yet … half of you, including some who wrote that RFK Jr. might be a Teflon secretary, figured that Kennedy would end up serving less than the average Trump appointee. Not sure if that’s wishcasting or what. (For what’s worth, I’m taking the over.)
Here’s how the numbers came out.

One of the big questions about the Medicare Part D drug benefit, as it enters its “IRA phase,” is what will happen to patient out-of-pocket costs. As a reminder, the overall structure of the IRA is not designed, in particular, to save patients money but rather to save the government money.**
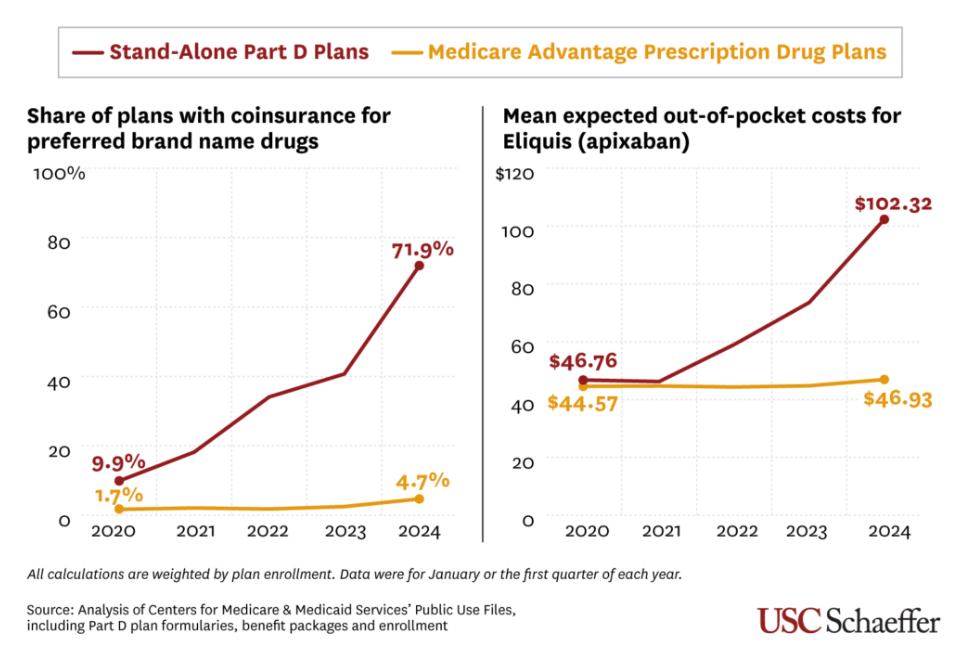
There is new data from a JAMA study out on Friday that suggests that patients ought to watch their wallets. Over the past five years, patients in standalone Part D drug plans have seen a massive shift from fixed co-pays to coinsurance based on the price of the medicine. That’s driven out-of-pocket costs up, from an average of $47 to $102 a month.
The same phenomenon has not been present in Medicare Advantage drug plans, which have more ways of offsetting drug prices.
Here’s what that looks like graphically:
Here’s how USC’s Erin Trish, who led the study, put it: “Medicare beneficiaries are often blindsided when they suddenly have to pay much more for the same drug they may have been taking for years. While Part D’s new out-of-pocket cap will help beneficiaries over the full year, that initial sticker shock could make it harder for them to maintain their prescription, potentially leading to worse health outcomes.”
It’s elegant work, and it informs all kinds of questions, from “Can we expect seniors to bear more and more OOP in Medicare?” (where the answer appears to be “yes”) to “Are standalone Part D plans viable?” (where the answer, for a lot of reasons, is “maybe not.”)
** There is a giant exception here, which is patients who hit the $2,000 out-of-pocket cap, and that should not be minimized. It is absolutely life-changing for a lot of beneficiaries. But for everyone else, the benefits are less clear.

I’m still working through the “what to do” question when it comes to the assault on science. It was another rough weekend.
In the short term, “what to do” means rooting for the lawyers. In the long term, it means contacting my lawmakers.
In the medium term, my assumption is that sunlight will help.
Understanding what is at risk from a research or oversight or regulatory point of view is important. In that vein, there are a lot of reporters looking to illuminate these topics.
So here are some reporters who have put out public calls for assistance in their efforts to dig into stories about firing and at-risk research dollars. If you have a story about what’s going on, please consider telling it. I can vouch for them all:
Rachel Cohrs Zhang, Bloomberg
Matt Herper, STAT
Lisa Jarvis, Bloomberg
Eric Strauss, ABC
Nyah Phengsitthy, Bloomberg Law
If you know of other reporters (or are another reporter!) who have asked for help as they sniff around these topics, let me know and I’ll amplify those as well.
***
I’m challenged somewhat by my scope here. This isn’t a newsletter, really, about research or public health or regulatory science, except insofar as it intersects with the underlying economics of the health care system, and I’d quickly be ground down if I committed to opening the aperture on Cost Curve too much broader.
At the same time, “the underlying economics of the system,” are pretty well intertwined with “research or public health or regulatory science,” so I can’t exactly just turn my head and continue on my merry way.
So my goal will be to aggressively curate news where that overlap is clear, as well as flag other thoughts to the broader “what to do” question when I have something to add to the dialogue.
If you have other suggestions, I’m here.
I am a huge fan of wildly implausible visions of how the U.S. health care system can be rebuilt from scratch because the questions raised and holes in the logic are hugely instructive in their own way. Mark Cuban took on this task last month, and singer/songwriter/business guy D.A. Wallach just published his audacious vision. Do I think that we’re going to move health coverage to the blockchain and disintermediate insurance companies? Um, no. But I can’t wait to hear the conversations that this spawns.
This is a fantastic summary -- in JAMA Health Forum -- of state-level 340B transparency efforts, with a special focus on what’s happening in Minnesota. The assessment is led by the University of Minnesota’s Sayeh Nikpay, who knows this topic better than anyone. Minnesota’s first version wasn’t perfect, but they’re figuring it out. Here’s hoping that other states learn those lessons.
Cost Curve is produced by Reid Strategic, a consultancy that helps companies and organizations in life sciences communicate more clearly and more loudly about issues of value, access, and pricing. We offer a range of services, from strategic planning to tactical execution, designed to shatter the complexity that hampers constructive conversations.
To learn more about how Reid Strategic can help you, email Brian Reid at [email protected].
