

On Thursday, I said that Cost Curve would be off until Monday “unless someone misbehaves.” I don’t know why I put that evil on myself. Because, sure enough, someone misbehaved.
***
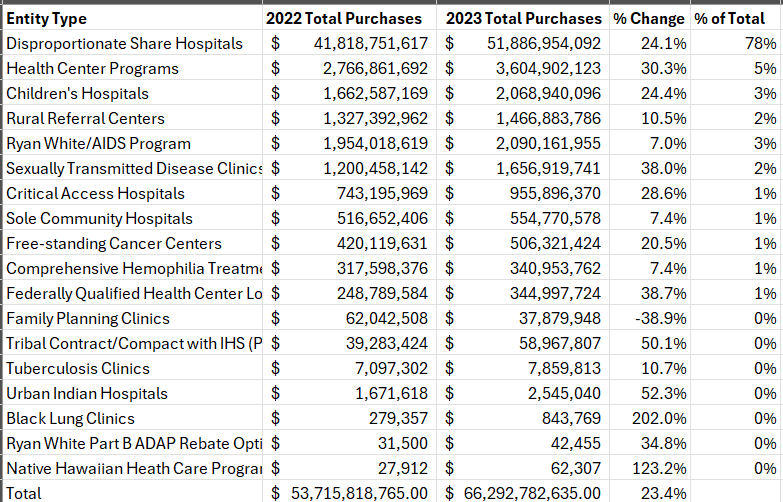
I’m interrupting your weekend because yesterday was the biggest-deal day of the year for 340B wonks, and I didn’t want it to go without special notice. HRSA dropped its annual numbers for the size of the 340B program, and they’re big.
Real big.
$66 billion big.
Twenty-three percent year-over-year big.
First, the background: You can see the HRSA data yourself here, and here’s what the year-over-year calculations look like:
Adam Fein has the historical numbers at his fingertips and has a LinkedIn post showing the long-term growth. (He’ll have a deeper dive soon, and I’ll link to that, too.) Ed Silverman at STAT was nice enough to quote my first impressions in his story yesterday. If there’s additional commentary, I’ll include in Monday’s Curve.
I had six initial reactions:
As I mentioned to Ed, the HRSA data suggest that the program is growing faster than pretty much anything else in health care, but we have zero idea where all of that money is going. There’s a tremendous amount of research that has looked for connections between 340B dollars and charity care, especially for DSH hospitals, and failed to find anything. Where, then, is all of this money going?
The DSH hospitals account for 78% of the 340B purchases, and those hospitals bought $10 billion more 340B drugs in 2023 than in 2022. This isn’t a new trend, but it’s a reminder that the issues with the program’s growth and the lack of accountability aren’t around community health centers or other specialized covered entities. This is a big-hospital thing.
This makes pretty clear that hospital claims that contract pharmacy restrictions are causing grievous harm are generally overblown.
For the first time, HRSA released information on which medicines are most often purchased at 340B prices, with Keytruda and Biktarvy topping the list. That data is eye-opening.
It’s astonishing how much of Keytruda’s sales are moving through the 340B program: HRSA said that there were $6.9 billion in Keytruda sales in 340B. For context, Merck reported U.S. Keytruda revenue of $15.1 billion. So 340B sales accounted for 45% of the net revenue of the therapy.
I plan to have that analysis for all of the top 10 medicines in Monday’s edition.
The drug-specific data also suggests that a reckoning is coming for hospitals relying on 340B dollars. The top three medicines on the list are all due for IRA “maximum fair price” in the 2028 cohort.
Because the IRA doesn’t allow for both a 340B discount and a MFP, the billions in 340B arbitrage now generated by those medicines will disappear, creating a gaping revenue hole for hospitals that have come to see 340B as a cash cow. (Remember, these medicines are not only bought at a discount, they’re also massively marked up.)
We’ll get a preview of the problem with the first price controls hit in 2026, but the fact that none of the first meds to have been “negotiated” made the HRSA top 10 list suggests that the impact of first round is going to feel like a gentle summer rain compared with the tsunami that may hit a couple of days later.
It’s only going to get hotter under the spotlight for hospitals. This Guardian piece from Friday is an absolutely brutal takedown of how one hospital system in Indiana is jacking up prices even as it goes after uninsured patients for six-digit medical bills.
The system, Parkview, includes 340B hospitals, but the piece doesn’t even get into the 340B element. But every Parkview -- every hospital with a “servant leader” making $3 million with charity care levels that are low and falling -- is at risk of being asked a tough question: where are the 340B dollars going? To date, hospitals don’t have good answers to that.
All of this will foundational to the coming debate about whether 340B is truly helping patients and whether there might be a more thoughful way of ensuring both hospital sustainability and support for vulnerable Americans than an opaque system that’s growing expontially with almost zero accountability.
