

Jeez. Lots to blow through for a Wednesday morning in July. Buckle up.

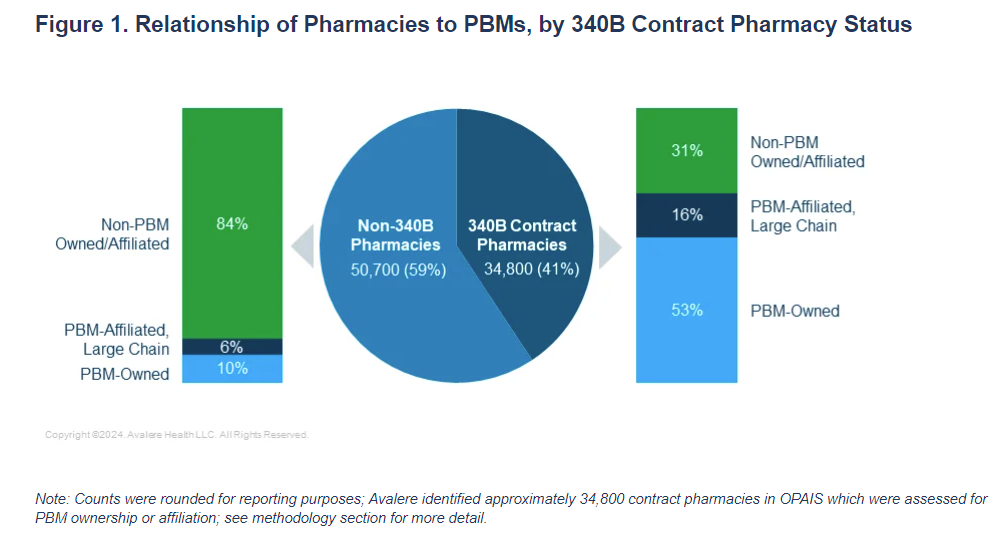
Late-breaking news. I’ll talk more about this tomorrow, but Avalere/Community Oncology Alliance have a great study out that shows just how closely tied PBM-affliated pharmacies are to the 340B program. You can read the report here.
My gut says that wherever you stand on 340B, you probably feel uncomfortable with the idea of the program padding the bottom line of PBMs.
There are two ways that the PBM industry can get reeled in.
One is government regulation. We talk about this all the time around here. Figuring out the right policies at the state and local level to boost transparency and bar abusive practices is an intellectual feast for wonks.
It’s also of dubious effectiveness. Getting laws passed is hard, and PBMs have shown themselves to be quite adaptable, prepared to evolve around any hurdles that might get erected.
The second way to lessen the market power over PBM is to get their clients -- the health plans -- to drive a harder bargain by demanding better prices, lower fees, or more transparency. This, too, has been pretty tough. These are big, complicated systems, and there are a lot of forces pushing corporate decision-makers away from rocking the boat.
But there is one opposing force that is growing in prominence: the threat that if a company’s health plan gets lazy in how it picks a PBM, it’s going to get hauled into court by its employees. Health plans have a fiduciary duty to pick a PBM that delivers a good deal, and that duty was supercharged by the Consolidated Appropriations Act of 2021. (That’s “CAA,” in wonk parlance. You’ll be hearing that abbreviation a lot more.)
Anyway: all of this is prelude to flag a second lawsuit dragging a large employer for making questionable decisions about its pharmacy benefits. Four former employees of Wells Fargo have filed a class-action suit spotlighting the ways that the Wells Fargo plan happily paid hugely inflated costs for generic drugs, per its contract with Express Scripts, sticking employees with big bills.
If that storyline feels familiar, it’s because it mirrors almost identically a suit brought against J&J earlier this year.
I won’t go too far into the weeds on the specifics. For a more detailed overview, STAT’s coverage is good, and Bloomberg broke the news. If you’ve got a couple of hours, though, the suit itself is great reading.
But I’ll make a couple of additional points.
First, the Wells Fargo suit is a little different from the J&J one in that there is an allegation that Wells Fargo -- in addition to overpaying for generic meds -- also paid Express Scripts absurd fees: $25 million a year, or $135 per beneficiary.
That’s a public number, BTW, and I suspect a lot of HR departments are going to be trying to figure out how much in fees they paid last year. I did some poking around in the public filings and there are definitely some companies that might be nervous. Not a great morning at Kohl’s, I would think.
Second, it’s worth noting that the same law firm is behind both the Wells Fargo suit and the J&J action. That firm, Fairmark, has ties to Arnold Ventures. I’m not suggesting that Arnold is underwriting this or casting any aspersions. Just flagging that these folks believe in system change via the legal system.
All of this to say: this isn’t the last we’re going to hear of this topic. Stay tuned.
This is a smart piece in Health Affairs Forefront arguing that CMS should adopt a broader definition of “unmet medical need” under the IRA. Right now, unmet medical need only encompasses clinical benefits, but that’s a fairly myopic way to look at benefit.
The authors -- from Tufts and Genentech -- suggest that considering access and quality of life, among other element, would help better align IRA decisions with what’s really important to patients.
Elsewhere:
This is kind of a weird Boston Globe story on the possibility that 340B reform will harm community pharmacies. At least, I think that’s the point. It’s telling the story through a pharmacy directly affiliated with a clinic, which is the kind of 340B beneficiary everyone -- without exception -- wants to protect. But the broader implication is that 340B reform would hurt pharmacies … and no one thinks that the 340B program was designed to subsize pharmacies, community or otherwise.
More earnings. Merck was silent on policy topics, but Pfizer weighed in on the IRA, calling it “a piece of legislation that clearly is harmful for supporting research and development in the sector” and “a very big loss for innovation and for the crown jewel of American industry, which is the life science technology business.”
Speaking of earnings, Axios is the latest to try to summarize the industry’s position on the IRA, focusing on the “manageable” impact of the first set of price controls but elevating comments on broader concerns.
STAT flagged seven people who might drive health policy in a Trump administration.
I cannot endorse strongly enough this STAT First Opinion by a Philadelphia doctor who believes that medical school students should be taught how to address with patients cost concerns in health care. I have long had a dream that a client would ask me to help design educational programming to help doctors better understand value … and better help patients, and the STAT piece provided a great outline for what that could look like.
Thanks for reading this far. I’m always flattered when folks share all or part of Cost Curve. All I ask is for a mention or tag. Bonus points if you can direct someone to the subscription page.
