

Thanks to everyone who weighed in on the future of Cost Curve yesterday. I’m keeping the survey open for another day, so if you haven’t clicked over, I’d be appreciative if you took a look.
I’ll provide a roundup of your feedback later in the week, but -- for now -- please know that I don’t intend to change the core offering. The plan is to keep this newsletter free and this community growing.

The text of the big year-end spending bill is now public, which means that all kinds of political wrangling out in public is about to begin. I’ll spare you the process back-and-forth and go straight to what’s in the bill.
Here is a section-by-section summary of the bill. Here’s the whole thing, if you want to peep the actual language.
But -- because you are all busy people who aren’t going to click those links -- here are the relevant sections on PBMs:
Sec. 113. Preventing the Use of Abusive Spread Pricing in Medicaid. This section bans “spread pricing” in the Medicaid program, which occurs when pharmacy benefit managers retain a portion of the amount paid to them (a “spread”) for prescription drugs.
Sec. 227. Modernizing and Ensuring PBM Accountability. This section:
* Prohibits PBMs and their affiliates from deriving remuneration for covered Part D drugs based on the price of a drug;
* Requires PBMs to define and apply drug and drug pricing terms in contracts with Part D plan sponsors transparently and consistently;
* Sets out annual requirements for PBMs to report on drug price and other information to Part D plan sponsor clients; and
* Empowers Part D plan sponsors with new audit rights with respect to PBMs
Sec. 901. Oversight of Pharmacy Benefit Management Services. This section promotes price transparency for prescription drugs purchased by employer health plans by ensuring Pharmacy Benefit Managers (PBMs) provide group health plans and issuers with detailed data on prescription drug spending at least semi-annually. Such data includes gross and net drug spending, drug rebates, spread pricing arrangements, formulary placement rationale, and information about benefit designs that encourage the use of pharmacies affiliated with PBMs.
The section also ensures that health plans and individuals can receive a summary document regarding information about the plan’s prescription drug spending.
Sec. 902. Full Rebate Pass Through to Plan; Exception or Innocent Plan Fiduciaries. This section requires that PBMs fully pass through 100 percent of drug rebates and discounts, excluding bona fide service fees, to the employer or health plan regulated under the Employee Retirement Income Security Act of 1974 (ERISA) for new contracts, extensions, or renewals entered into for plan years beginning 30 months after the date of enactment. This section also clarifies the meaning of “covered service provider” under ERISA.
BTW: there is also a patent provision:
Sec. 904. Title 35 amendments. This section curbs so-called “patent thickets” by limiting, in certain instances, the number of patents that a reference biological product manufacturer can assert in a patent infringement lawsuit against a company seeking to sell a biosimilar version.
And there is a bit about allowing the National Academies to study the idea of having a “prize”-based incentive system for drug development, which I think is a Bernie Sanders thing in every sense of the word. (Sec. 634)
In a world of infinite time, I would have looked at these provisions, matched them to the legislation where they originated, and offered some perspective on what they’ll cost, how impactful they’ll be, and the like. Sadly, I don’t have infinite time today.
Instead, I’d suggest that the PBM provisions that are likely to be the most important are the ones that the PBM lobby is the most mad about. And that is clear: the PCMA statement on the big bill leans hard into their objection to the delinking language (Sec. 227).
There will be a lot more on this as the legislative process inches forward and more commentary emerges. But -- for now -- this is the state of play.
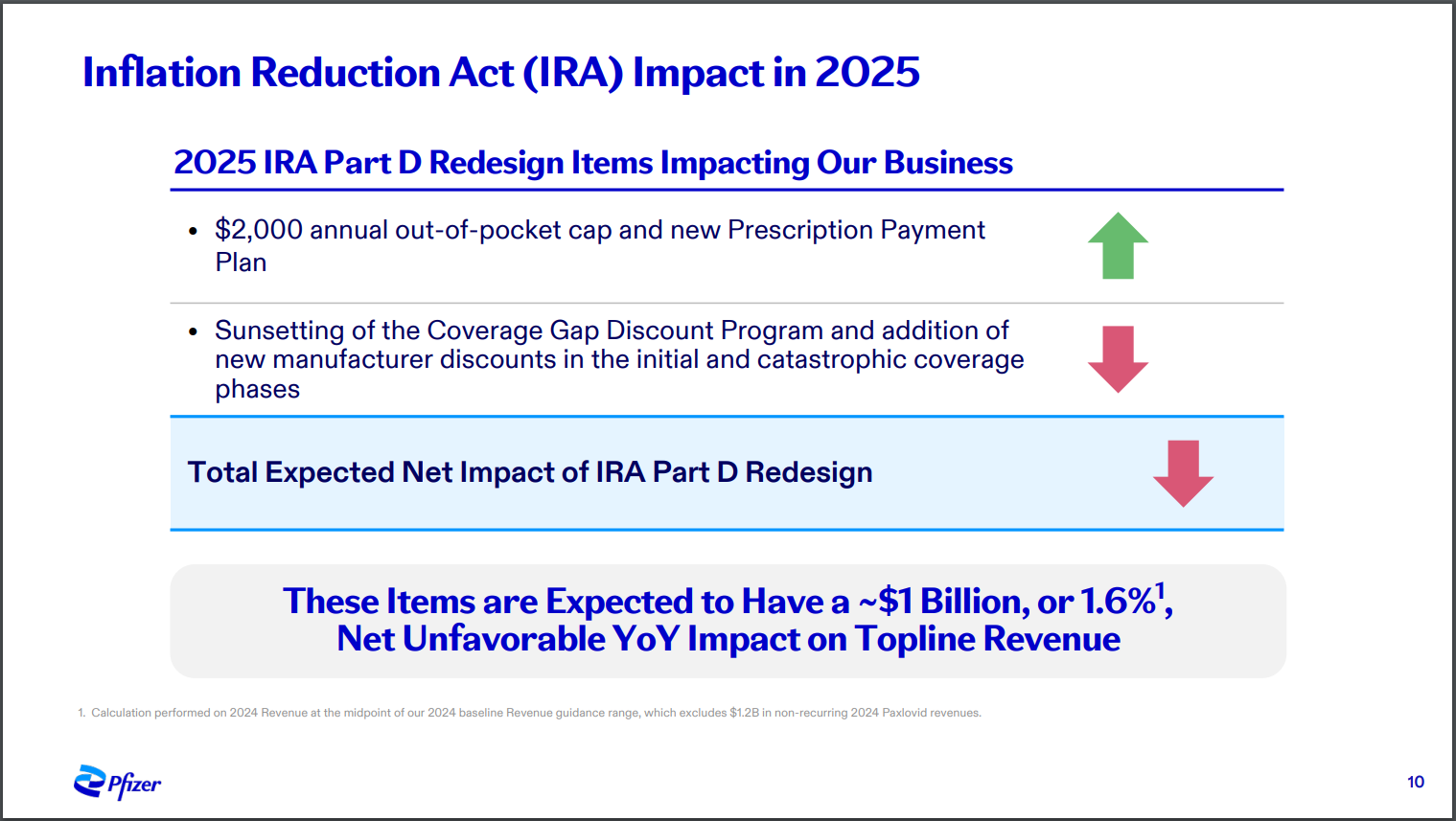
On another day, I would have made a much bigger deal about Pfizer’s disclosure that the Part D redesign portion of the IRA is going to cost the company one billion dollars.
The math: $1.5 billion in additional costs from those in the catastrophic phase, less $500 million in additional revenue from increased use of medicines because of the $2,000 out-of-pocket cap.
It’s worth nothing that the changes to the Part D benefit -- especially the $2,000 OOP cap -- have been broadly supported by the industry. Though there is real concern about price controls, I think that companies, in general, are OK taking a hit with redesign because it’s the right thing for patients.
ELSEWHERE:
On another day, I would have made a much bigger deal about this KFF Health News article, too. It gives a nice overview of the backdoor legal fight over PBMs: employees suing their employers over crappy benefit design. It’s a reminder that, for all the hype about PBM legislation this week, true impact on the PBM landscape will come from a multitude of directions.
This is a solid piece by Joe Grogan highlighting the unstoppable-force-vs-immovable-object conflict that will soon arrive around 340B. It’s clear that the CMS needs there to be some way of separating out “maximum fair prices” from 340B prices for the IRA. And it’s clear that HRSA, which oversees 340B right now, is not being solution-oriented. For the record, Adam Fein is putting his money on CMS in this fight, and it’s unwise to bet against Adam’s predictions.
When No Patients Left Behind and Merrill Goozner agree on something, you should probably take it to the bank. Goozner has a STAT First Opinion declaring that the idea of “skin in the game” -- that cost-sharing somehow creates better consumers -- is a failure. Not much to argue there.
Cost Curve is produced by Reid Strategic, a consultancy that helps companies and organizations in life sciences communicate more clearly and more loudly about issues of value, access, and pricing. We offer a range of services, from strategic planning to tactical execution, designed to shatter the complexity that hampers constructive conversations.
To learn more about how Reid Strategic can help you, email Brian Reid at [email protected].
